Social policy in Greece in the interwar period: events, conflicts and conceptual transformations
“Social policy in Greece in the interwar period:
events, conflicts and conceptual transformations”
George Nikolaidis and Spyros Sakellaropoulos
ABSTRACT
This study gives an outline – by period – of the most basic social policy measures and health and welfare programmes of the Venizelist political centre. The periodization involves a breakdown of the abovementioned policy into three separate phases whose distinguishing characteristics are then outlined - namely a first period from 1910 to 1916 where the predominant feature is the attempt to develop a range of structures and services that might begin to try to cover the growing needs of the population of a geographically expanding Greece. In the second period between 1918 and 1920 this expansionist strategy of the social state would come to be regarded as too advanced by the Venizelist centre itself and on the basis of forms of social and political expression including some previously developed inside the working class, attempts would be made to roll it back. In the third period between the years 1928 and 1932, which were to be marked by a greater sharpening of social conflict, the politics of the Liberals were to involve endeavors to carry out bourgeois modernization as a counter to the social crisis, efforts conducted in a spirit of pragmatism in a situation where a whole array of economic, social and political parameters were limiting the potential for promoting implementable policy measures at that time. Moreover, in this final phase, all such social policy measures were characterized by obvious efforts to manipulate and control the political and social forms of organization of the popular classes.
Starting from the above considerations, our analysis seeks to distinguish itself from views particularly prevalent among Greek politicians even today, as well as among sections of the electorate, that portray Venizelos as a representative of advanced social radicalism. But we also distinguish ourselves from those who regard him as an exponent of bourgeois modernization. While the former view perceives Venizelos’ policies as part of a continuous linear course towards progress, the latter sees everything as the outcome of a bourgeois class strategy for modernization of economic and social processes. Both stances suffer from an inability to comprehend that social evolution develops unevenly and above all is the product of social balances of forces that are overturned, modified, transformed.
“Social policy in Greece in the interwar period: events, conflicts and conceptual transformations”
George Nikolaidis and Spyros Sakellaropoulos
- Introduction
In this paper we shall attempt to show that the adoption of the first forms of social welfare and health care policies by the governments of Eleftherios Venizelos is merely one variant of a general rule characterizing the developmental course of the Welfare State in capitalist countries, i.e. it represents the historical transmutation of an institutional formation that is contradictory in terms of its social (class) content.
What we maintain is that social expenditures have a dual function. On the one hand they of course comprise gains of the dominated strata, the fruit of intense social struggles. But on the other hand the State has managed, step by step, to incorporate its own objectives, with the greater part of these expenditures serving the needs of capital reproduction. Specifically, in the field of health, these goals embrace the functions of regeneration of labour power, reducing the cost of its reproduction in the case of public expenditure on health, defense of the interests of specific sections either of capital (private health care organizations and companies producing and dispensing medical and pharmaceutical products) or of the broader social bloc of the dominant classes (including, e.g. medical doctors). They also include pursuance of social control through regulation of the roles of the “healthy” and the “sick” (Waitzkin and Waterman 1974: 36-64, Navarro 1975: 183-196). The phenomenon is thus contradictory: the content of its functions are both the result of and the starting point for social struggle (Gough 1979: 14).
Naturally, as will be understood, our position on the welfare state and more concretely on the Venizelist political centre is the corollary of our overall position on the role of the state in contemporary capitalism. Contrary to views interpreting the state as a simple “neutral” instrument of class power and other conceptions which see it as a relation between social classes, we present the State as the outcome of class struggle within a mode of production. The class identity of the State is inherent in its creation within each productive system - the latter is after all the matrix within which it comes into existence. Thus, within the capitalist system, the goal of the bourgeois State is to give long-term representation to bourgeois class interests. The overall concern of the State is evidently not something static but continually takes account of modifications in the intra-bourgeois power balance, the upgrading and downgrading of sections of capital, the totality of expressions of class struggle.
2. General outline of international tendencies and policies on health, welfare and social policy after 1900
In the field of health the inherently contradictory character of public health measures had become evident as early as the 19th century and indeed through the activity of outstanding personalities from the world of bourgeois politics and from the international academic community. Characteristically, on the one hand the founder of the cellular conception of the human organism, but also leader of the liberal opposition to Bismarck, R. Virchow, declared as early as the mid-nineteenth century that “the physician is the natural advocate of the poor”, that “politics is medicine on a broader scale” and that “medicine is a social science” (Silver 1987). On the other hand, Lord Balfour declared with revealing perspicacity in 1895 that “social legislation is not just something different from socialist legislation: it is the most effective antidote to it”. Similarly, in one of the first British manuals on workers’ medical problems, in 1925, there is an explicit (and premonitory) record of the remark that “…chickens, racehorses, circus monkeys, are fed, trained and kept at the peak of their physical abilities, so that the productivity of their particular functions will reward our efforts. The same principle applies for human beings” (Rodberg and Stevenson 1977). This reparatory role of social policy and public health measures was of course something with which its own protagonists were entirely familiar. Thus, for example, as typically recorded by a contemporary observer “even when in 1847 the Prussian government sent Virchow to investigate the typhus epidemic in Upper Silesia”- an investigation which led to the compilation of a report that Virchow himself considered his most important contribution to medical science (Ackerknecht 1998: 193-195) – “the government was trying to exert repression on the masses of the peasant population crowding into the farms of the Junker landowners, whom it was supporting” (Elling 1994).
Although the contradiction indicated above between the reproductive utility for the ruling class within the capitalist mode of production of the public health measures and the related popular demands and gains in many ways remains the most basic of the active contradictions within the social policy measures, other secondary contradictions also coexist with it, undergoing a parallel evolution. One of these is the organic contradiction between the repressive and the protective character of the policies under implementation. Thus, as early as the beginning of the 19th century, when the first manual of preventive medicine was published, J.P. Frank had clearly outlined the repressive character of any likely intervention. “State power, as expression of the general will of the community, bears the overall responsibility for each concrete individual and should therefore maintain constant supervision of people from the cradle to the grave,” he says in his in any case most eloquently entitled work: “A comprehensive Medical Police Force”. On the other hand a number of organizations such as trade unions, local authorities, associations and scientific bodies promoted the idea of society as a whole being responsible for securing a healthy environment, particularly for the social classes for whom such an environment is a vital necessity (Bale 1989). In this historical period, the repressive aspect of social policy and public health measures played a conspicuous role in shaping dominant political orientations, particularly in the imperialist centers, which felt threatened by infectious and contagious diseases, both in country areas and in the overseas possessions of the big European states.
Another secondary contradiction characterizing this period is the position of the medical profession and of the hospital as a structure within the emerging health care system. It had already become evident from previous forms of social organization that there is a special relationship between the medical profession and political and ecclesiastical power. A. Gramsci characteristically observes that “between medicine and religion there have been, and there continue to be, links in the form of certain organizational functions, quite apart from the fact that wherever the doctor puts in an appearance, the priest also shows up. Many great religious personages were, and were considered, great healers; cf. the idea of the miracle and resurrection of the dead. Even at the level of royalty the idea long prevailed [until after the Middle Ages] that they were able to heal simply by laying their hands on the patient, etc.” (Gramsci 1949: 55-56).
These relationships were naturally transformed in accordance with the concrete historicity of the individual social formations and the social conflicts that correspondingly arose. Quite frequently such conditions had over-determining consequences for the particular forms assumed by the various policies that were pursued in the countries of Europe and North America. Thus, on the one hand, e.g. in the United States, the conflicts – often of doubtful scientific merit and validity – between itinerant popular healers and the up-and-coming grouping of scientific hospital medicine (whose effectiveness nevertheless did not seem noticeably superior to that of its opponents) were settled through centralized repression by means of the notorious Flexner Report (funded by the Carnegie and Rockefeller foundations) – a report that made possible a suffocating control of medical staffing and the definitive hegemony of hospital medicine (Baer 1989, Fox 1986). On the other, in Europe the conflict was probably internalized within the body of professional medical cadres, leading to a polarization of the latter firstly into layers practicing their profession within newly established social-security organizations and secondly into layers confined to private medical practice involving only a small part of the population (Honigsbaum 1990). This internalization led both to a proliferation of the attendant conflicts (between the prospect of measures of universal social policy and their rejection) throughout the political strata of the various states and to the elaboration of a range of differentiated political positions on social legislation within the conservative and liberal currents. The example is well-known, for example, of Lloyd George’s clash with the conservative Dr. Cox over the National Insurance Act 1911-1913 in Great Britain (Bayum 1988). The disagreement should nevertheless not be seen as typical of a more general dispute between liberals and conservatives over social policy. Though in most cases it was the liberals who proposed the institution of measures for public health and social welfare (Virchow himself led the liberal opposition to Bismarck, losing his university chair for his participation in the insurrection of 1848), the confusion of roles, attitudes and positions that prevailed at the time was much broader. This historical period saw the emergence of conservatives adopting stances favorable to the social state (for example it was Bismarck, finally, who with the Decree of 17/11/1881 and the other decrees that followed it[1] established the model for the social-insurance health system that remains in force to this day in most of Europe and many other countries in the world – Skoutelis 1990:27) and also of liberals expressing opposition to such a prospect.
During the same period a radical modification took place regarding the character of medicine and the way it was practiced as well as of the manner of dispensing health services. Whereas, that is to say, for a period that had lasted for over two centuries, hospitals had been primarily places of refuge, institutions which - although philanthropic in character – had administered inferior-quality health care to the poor, with the more affluent social classes (and whoever possessed the necessary means) systematically preferring home treatment, at this point in time the character of the hospital underwent drastic change. The incorporation of (laboratory-based) technological innovations into diagnostic and therapeutic practice, and indeed the prestigious achievements of the time in physics and chemistry, helped prepare the ground for rapid growth of the hospital sector as a now upgraded locale for health provision. In the most developed countries the hospital began to rise above its previous associations with manifestly charitable and palliative functions (Ackerknecht 1988: 255-275). The use of the white tunic by medical personnel (even doctors working outside the laboratory) became generalized, as part of an endeavor to secure the same acceptance as that enjoyed by specialists in the key sectors of natural science. Various forms of collective medical practice for profit made a dramatic entry onto the scene (Pefanis 2004: 133-170). Thus, while in the mid 18th century, for example, popular prejudice had seen admission into the hospital as something to be shunned, suggestive of penury and ominous in its implications, in the first decades of the 20th century a polar shift in attitudes took place, generating subsequent social pressure for construction of ever more hospitals in the countries of Europe and North America (Abel-Smith 1964, Knowles 1973).
The conglomeration of conflicting conceptions and practices, not to mention the way in which they were also reflected, in part, in the legislation of various countries at the turn of the 20th century, may go some way towards explaining popular distrust of advanced forms of medical treatment (Honigsbaum 1990). Over time this distrust does seem to have undergone transformation and to have receded with the increased prestige of the dominant conceptions and the prerequisite establishment of a homogeneously functioning centralized state. Thus in countries with a history of strong central authority buttressed by an entrenched ideology, this type of contestation subsides and is reintegrated smoothly and rapidly. This transition was naturally effected in an over-determined setting by means of an ideological subtext of scientism, hegemonic at a common-sense level, and by acceptance and assimilation of its outlook by the upholders of political and social order and the subordinate social classes. By contrast, in social formations where the predominant school of medicine is imposed “from above”, predicating dissolution of older therapeutic paradigms, and where the state is constituted through operations both more repressive in character and federalist in origin, without conspicuous involvement in everyday functioning (e.g. in the U.S.A.), these challenges to the dominant medical model would persist, metamorphosed into every manner of “parallel” alternative health-care practices with comparatively significant penetration, particularly among the popular strata (Ehrenreich and English 1979, Baer 1989, White, 1990).
- Greece at the turn of the 20th century
However dramatic, the evolving health, welfare and social policy situation in Greece proper in the early 20th century, it nevertheless presented aspects of all aforementioned contradictions. Figures of health statistics for the Greek population were among the worst in Europe and the legislative framework non-existent, given that since the time of the Bavarians’ reign in Greece no new relevant legislation had been passed. Implementation of preexisting institutional framework was deficient, primarily covering Athens and almost nowhere else in the country supported by only minimal funding available for the purpose. At the turn of the 20th century the basic legislation covering health issues in Greece consisted of the Royal Decree of 01/12/1836 “On the Administration of Eleemosynary Establishments” and the Royal Decree of 21/12/1836 “On the Municipal Police”. Under the general provisions of the Bavarians for public administration in Greece, municipal authorities and philanthropic organizations exercised the key responsibilities on questions of hygiene, with the individual foundations being administered by some of the corresponding affiliated municipal councils. Protection of public health in a more general sense was entrusted on one hand to the police and on the other – where scientific expertise was required - to the Doctors’ Conference. There were few scientifically trained medical doctors in the country, mostly coming from the upper strata of society and situated in the urban centers. Despite this fact, from the very outset (i.e. the 19th century) there was a heavy popular demand for training in medicine, chiefly because of the high earnings the medical profession could command, notwithstanding the vehement condemnation directed against it on that account by the press of the day. At the same time, particularly in the provinces, quacks and “empirical” doctors with dubious qualifications carried out therapeutic tasks for the mass of the population. Functioning hospitals, mostly charitable in character and under municipal supervision, were very few in number; conditions in them were terrible and the standard of health services they provided was equally low. Despite the importance theoretically attached to it as a means of protecting children, welfare remained at rudimentary levels (Kalliga 1990: 225-234); there were numerous claims e.g. that the high levels of mortality in the nurseries and homes for the elderly of the time were primarily the result of the wretched prevailing conditions and the rough behavior of personnel. Popular attitudes, as it is evidently recorded in various texts of contemporary literature, were characterized by generalized distrust of scientific medicine, while there is no shortage of testimony demonstrating laymen’s preference for “quackery”.
It should be also noticed that the overall orientation of the academia during the period under study was characterized by several contradicting views prevailing in Europe at the time being. For instance, academics like A. Christomanos, Professor in Athens’s School of Polytechnics, were publicly contradicting views on the necessity of hygienic reform of Athens’ obsolete sweeping system on the grounds of a rather questionable report confirming the quality of water and refuting its implication in typhoid epidemics (Mavrogonatou 2008; 209). As far as medical academia is concerned, it seems that at least for the first years of Venizelist administration, it was mainly focusing on the battle against empirical doctors and its legal institutionalization as well as on issues regarding centrally regulated fees for medical services (Kapanidis 1988: 86, 94-5); while on the later years of Venizelos’ era a good portion of academics in Medical School of Athens were highly influenced by eugenics’ various doctrines focusing on the necessity of reversing the impact of the notion of “counter-selection”, viz. the increased surviving opportunities for the weakest members of society provided by civilization and its amenities including introduction of social legislation (Troumbeta 2008; 336). Those advocators like Prof. Moutousis and Prof. Koumaris were regularly crusading against social protection measures for the poor and in favor of repressive legislation forbidding marriage between the sick that could result in degenerated children. Among those was also one of the key figures of the Venizelist associates, serving also as one of his Ministers of Health, Dr. A. Doxiadis. On top of these, the overall medical opinion was also contradicting reforms like the introduction of social security defending free choice of doctor from the patient and afraid of a potential decrease or at least regulation of medical income (Zilidis 2008: 143).
Of course within medical doctors of the time being as well medical academics there were fierce advocators of the introduction of social welfare measures like Prof. Savvas who being rather disappointed by the lack of public health perspective within Medical School of Athens founded the Anti-Malaria League and became one of the founders of Athens’ School of Hygiene (Levett, 2008: 114-5). These voices were supported in due course by other prominent figures like doctors campaigning for the hygiene necessity of modernizing sweeping system of Athens (Mavrogonatou 2008; 208-9), criminologists contradicting bills for mandatory sterilization of people suffering from infectious diseases (Troumbeta 2008; 345, 349,351-2) or social theorists advocating for the socially beneficial character of health and social services. It is indicative of the tensions inflicted that all these aforementioned forces in favor of social welfare legislation along with Venizelos’ political leadership often had to call into international agencies and organizations to support their policy reforms. Such interference was invited on several occasions given also the troubled social context of Venizelos’ era (constant war conflicts, massive immigration and consequent humanitarian crises) as well as the overall prevailing approaches in the international scenery; these interventions included organizations and agencies such as the Rockefeller Foundation, the Nation’s League, Milbank Memorial Fund, the International Red Cross, International Labor Organization, some of which were often being contradicted by the local medical society (Weindling, 2008: 80-82, Zilidis 2008: 143-4).
To sum up, it seems that Venizelos’ administration comes to power at a time in which pre-existing capacity of the Hellenic state in health and welfare sectors was quite limited; additionally, socio-political circumstances increased needs to be met dramatically while necessary reforms towards modernization were received with controversial attitudes. The slow emergence of a trend in the direction of change, linked to a variety of socio-political transitions in the course of the period under discussion, acquires altogether different qualitative characteristics in the light of political reforms undertaken by Venizelos, which may be assigned to a number of different categories depending on the governmental period. The first period is distinctive for the numerous indications of support for establishment of a series of laws promoting the institutional framework of State intervention in social welfare, restructuring of the operational mode of the medical profession and recognizing the state’s responsibility for the supervision of public health (with Law 346 of 1914). The main factors generating the necessity for a new supportive social framework were the expansion of Greek national territory following the incorporation of Northern Greece, Epirus and Crete, the contraction of the agricultural population from 75% of the total in 1870 to 57% in 1920, with the number of urban workers rising from 7,300 in 1867 to 60,000 in 1909 and the repeated involvements in war operations (the Balkan Wars, the First World War, the Asia Minor Expedition). The breadth of coverage of this supportive social framework was later deemed too advanced and the development of the workers’ movement led to attempts to curb it between 1917 and 1920 (second period). It was nevertheless during this period too that a series of health and welfare measures were taken, the most important being the measures that would culminate in the establishment of the Health Ministry in 1917 (subsequently to be renamed the Ministry of Health and Social Welfare) and the legislative framework of medical care and social assistance for refugees. The third period (1928-1932) was to be marked by the worsening of social inequalities along with a numerical increase of the available workforce due to the simultaneous decrease of the rate of emigration from Greece and the entry of refugees into the Greek labor market. This period was also characterized by an attempt to reorganize the state’s health foundations and above all the creation of the Social Insurance Foundation (IKA). Nevertheless, even this last-mentioned specific legislative action suffered from numerous weaknesses: lack of state funding, absence of provision for unemployment and long delays in its practical implementation.
In light of the above considerations, we shall seek to distinguish our views both from those (particularly prevalent even today in Greek political circles and sections of the electorate) portraying Venizelos as an exponent of an advanced social radicalism, and from those that label him as a symbol of bourgeois modernization (Mavrokordatos 1988, Hatzijosif 1988). Our reason for making this distinction is as follows: while the former view sees Venizelos’ politics as a continuous linear course towards progress, the second explains everything in terms of the bourgeoisie’s strategy to modernize economic and social processes in Greece. Neither perspective grasp the fact that social development takes place unevenly and is at bottom-line the outcome of the balance of social forces, which can be overthrown, modified and transformed.
3. The period between 1910 and 1916
It is rather the case that during the first period of Venizelos’ administration (1910-1916) an original attempt was made to introduce state intervention into the relations between capital and labor. This enterprise aimed at bringing about a series of moderate institutional transformations with the potential of a) curbing certain excesses on the part of employers b) putting the country on a course of convergence with the advanced European societies c) confining all the changes within specific limits – such that they did not cause any problems for the process of economic accumulation or for entrepreneur profitability (Liakos 1993: 443).
It is worth mentioning that these governmental plans met with considerable resistance from representatives of business circles. The Review of Enterprises and Light Industry launched a barrage of invective against Venizelos; the Federation of Enterprises and Light Industry made repeated representations to him, arguing that the labour legislation had been voted “hastily and impulsively”, that it encouraged workers to be greedy and created problems in a country where “there is no social differentiation” (Fountanopoulos 199: 202). Addressing the Society for Political Science and Statistics in 1916, the Piraeus industrialist Economides asserted that “Some laws have been instituted for the protection of workers, in part necessary and beneficial, in part injudicious and damaging. There must be industry if there are also to be workers… The welfare of the workers must proceed in parallel with protection of industry”.
Among the politicians the more conservative voices expressed similar sentiments. For Theotokis workers were in any case not subject to exploitation and most strikes took place for no reason. He was moreover unable to see any reason why children should not work. Rallis was opposed to legalization of strikes, postulating an “indissoluble partnership” between workers and their employers. Gounaris judged the economy to be so underdeveloped that there could be no basis for a theory of contending classes. The parliamentarian Georgios Kantianis maintained that in Greece there were no workers, capitalists or labour movement “but some people come from Europe, or listen to what is said in Europe, and having no ability to judge or compare, infect us with an illness – because an illness is what it is, both there and here. They come to inject this sickness into the healthy, robust and flourishing body of our community, to overturn a dispensation from which we have until now derived only benefits. They come to….instill suspicion, distrust and hatred between employers and employees” (Hering 2004:929).
Venizelos’ answer to these criticisms was that “if we do not make these legitimate concessions to the workers today, tomorrow they will take much more from us through revolution (mentioned in Kordatos 1972:232).
On the basis of the above, during this period, a whole constellation of measures were taken in respect of labour legislation. Thus, 1911 saw the establishment of the headquarters for the industrial inspectors, who were given the task of regulating working conditions. Around the same time a law was passed covering employees’ hygiene and safety during working hours. In 1912 a law was passed regulating payment of salaries and daily wages. The same year was also characterized by the passage of legislation on child and women’s labour that made it illegal for children under 12 to work, or respectfully for children under 14 if they had not completed their basic education. The same law provided for limitations on total working hours for children between 12 and 14 years of age (up to six hours a day) and children between 14 and 18 years of age (up to 10 hours a day and up to 8 hours on Saturdays and the days before public holidays). There was also a legal provision of mandatory rest breaks from work, and working on Sundays was not permitted for minors under the age of 16 and for women. Night work was also prohibited for women and minors under the age of 18 and there was also a ban on certain types of work and certain occupations. The same law established a number of minimum social welfare measures: mandatory employment booklets, obligation of employers to notify the authorities about minors and women that worked for them, and activation of the Corps of Labor Inspectors (Lixouriotis 1988: 216-217). Later on, in 1913 and 1916, decrees were issued establishing the midday break in certain branches of production. Two new laws were passed in 1920 and the provisions of the International Labour Conference were adopted regarding regulation of night work, which was banned in the industrial sector for children under 14. Nevertheless, both the absence of administrative and organizational support for the instantiation of the new legal framework as well as the existence of a large number of exceptions, e.g. for children working in their family business, and also of ambiguities, meant that its implementation was extremely deficient, if not non-existent.
In 1914 a new law attempted the codification of pre-existing labor legislation along with the establishment of Sunday as a non-working day; however, this law had several exceptions for numerous different business sectors and cities. Another law, also regarded as significant, was passed in 1915 by means of which the notion of compensation for a work accident was introduced for the first time. It was also determined that an employer was obliged to compensate a worker who suffered an accident at work, undertaking payment of his medical and pharmaceutical expenses (Tsiros 1997: 95 ff; Leontaritis 1980: 55, Liakos 1993: 386-387). However, in reality this law was a compromise between workers and employers: the prescribed levels of compensation were very much lower than it is calculated would have been imposed by a court of law; for many years there was no adjustment to the amount paid and the arrangement did not cover all occupations or all diseases (Liakos 1993: 390).
Last but not least, during 1920 the Greek government signed six international labour agreements that had been voted in Washington in 1919 and involved introduction of the eight-hour day (which was nevertheless not generally implemented until 1935 under the Papanastasiou government), limitations on women’s labour and child labour and unemployment and maternity benefits (Tsiros 1999: 119).
As far as workers’ self-organization is concerned, in 1914 the passage of law 281 on associations created a new institutional framework for trade unionism. The constitutional amendment of 1911 had already made it possible for co-operatives to be established without the permission of the authorities, and dissolved only after a judicial ruling. The most significant innovation of the law of 1914 was that it prohibited simultaneous participation of employers and employees in the same association, imposing this way certain limits on the logic of the guild. At the same time it protected Greek citizens’ right to freely enter into an association without prior permission from the authorities, while an association could be dissolved only after some or other violation of the laws and even then only by order of the courts of law (Tsiros 1997: 106ff; Moudopoulos 1981 231 ff).
What has to be noted is that this entire development took place under a very strict state control, in respect to the provision for supervision of associations’ operations in matters pertaining to their conformity with the law, their specific articles of member association and the management of their finances in the case of professional societies. It is characteristic that associations were obliged to submit to a supervising authority an annual statement of income and expenditures, an inventory of fixed and movable assets, along with a membership list. Moreover, the supervising authority had to be present at the associations’ assembly meetings to monitor the legality of their proceedings. Moreover, in the event that for whatever reason there were grounds for initiation of legal action, the supervising authority could depose the association’s governing body. Trade union activity, finally, was forbidden for civil servants (Moudopoulos 1988: 245).
During this first period of the Venizelist administration measures taken in the health sector were along the same lines as the aforementioned ones in the welfare sector. For example, one of the first modernizing steps taken by the government was, through Law 4063/1912, to institute a new legislative framework on terms and conditions of medical practice and hospital administration (1914), in consonance with what was being done during the same period in other European countries and in North America. The phenomenon being targeted by these immediate measures of the Venizelist administration was “quackery”, viz. the “empirical” practice of medicine, but there was also a focus on the problem of the expanding (see below) hospitals and other health sector institutions being staffed by individuals entirely unsuitable for their work. Apart from their unsuitable personnel these institutions also suffered from a serious lack of infrastructure, with potentially tragic consequences. As a result overall child mortality is reported at that time to have amounted to 30.4, 10.6 and 6.7 children per 1000 for the age clusters of 2-5, 6-10 and 11-15 year olds respectively, with general infant mortality at levels of 106 deaths per 1000 births in the cities (Kapanidis 1988: 42-3).
But the crucial turning point on the legislative initiative of Venizelos’ administration was undoubtedly the passage of Law 346 of 01/11/1914 “On the management of Public Health”, where for the first time in Greece the charitable and local dimension of health services was abandoned and the state acknowledged its responsibility at the national level. This law, which was drafted by K. Savvas, an Athens University professor and by that time President of the Medical Congress, was imbued with a spirit of state superintendence of the entirety of the country’s service sector by the central government. But due to the war and the related political instability, as well as due to the opposition it encountered and the lack of provisional resources (both human and financial) for implementing it, it remained a dead letter.
Overshadowed by war, this period was at the same time characterized as a period of expansion of hospital treatment. As mentioned previously, before 1909 most hospitals in Greece were public and/or charitable institutions with serious deficiencies in infrastructure and personnel. The epidemics, such as the cholera epidemic in Macedonia in 1913, eruptive typhus and plague in 1914, together with the Balkan Wars, rendered the situation tragic in most of them: overcrowded with patients who often slept on the floor, wretched conditions of hospitalization, prevalence of a multiplicity of infectious diseases precisely because of the overcrowding and the absence of even the most rudimentary hygiene. At the same time (as early as the first decade of the 20th century) an increase in the number of specialist hospitals began. Many hospitals were established between 1909 and 1916, such as the “A. Syngros” hospital (1909) and the Mt. Parnes Sanatorium (1914) in Athens, the “Loimodon” (infectious diseases’) hospital (1912) and the Psychiatric Hospital (1914) in Thessaloniki, the Psychiatric Hospital of Souda (1910), the Leper-house (1909) and Eye Hospital (1914) of Chios, the Mytilene Sanatorium (1915). Additionally, a number of previously functioning hospitals were considerably expanded, the most famous of which being the “Sotiria” Sanatorium, which received state funding for the first time exactly during this period. Other such institutions were the “Dromokaiteio” Psychiatric Hospital in Athens and the Spinalonga Leper Colony in Crete. It was at this time also, (1909), that the First Hellenic Tuberculosis Congress was held. Moreover, at the same time the Venizelos administration (both while it was in Athens and afterwards in Thessaloniki) funded several committees of distinguished citizens to undertake charitable work for the first wave of war refugees, as well as for the sick, wounded and crippled from the Balkan wars.
4. The period between 1917 and 1920
The restrictive measures included in the law of 1914 were not successful in repressing the workers’ mobilizations. The mushrooming of strikes during the period between 1917 and 1920 led to increases in wages, with the result that the Venizelos government was led to adopt further restrictive measures against working class trade-unionism (Liakos 1993: 444). Law 1207/1918 gave the right to the Law Council, and not the Court of First Instance, to dissolve workers’ associations if it was judged that their mobilizations of strikers endangered public order. This was a tangible regression from Law 281, where a strike was not grounds for dissolving an association (Liakos 1993: 166).
A little later, with Law 2151/1920, it was decided that, in the event of a strike, within two days a general meeting must be convened, where if one quarter of the regular members did not attend, the meeting had to be called again within twenty-four hours and if, again, there were not a quorum, the governing board of the association could not implement any decision for a month. The presence of representatives of the Greek Trade Union Confederation or other federations at the relevant proceedings was prohibited. It was also prohibited for individuals under the age of 18 to participate in secret ballots on strike-related issues, and restrictions were imposed on the right to stand for election (Moudopoulos 1988: 250-251; Liakos 1993: 167).
The same year, with the Royal Decree of 15/20 May, new restrictions were instituted such as election only of Greek citizens to administrative bodies of associations and the fact that among the grounds for dissolution were utilization of assets for other than statutory purposes, such as for example economic support for striking workers.
Essentially the establishment of the law on workers’ associations came as a by-product of the effort to modernize the country’s institutions given that the move away from what had until then been a purely agrarian economy created a qualitatively new situation. This is the reason that during the same period, 1914-1915, Venizelos implemented laws establishing commercial and industrial chambers, farming co-operatives and agricultural chambers. All these reforms, in other words, were attempting to prepare the ground for active intervention by the State in the differences between social classes and layers. When it was judged that these disputes had become particularly serious, there would be even stronger state intervention to prevent challenges to basic aspects of the regime of private property. As Venizelos himself asserted in the Parliament: “..this struggle for improvement of the day-to-day life of the working class will proceed in step with the genuine progress of the country when we succeed in extricating the workers from the clutches of their new exploiters.” And the reason for this was: “If in the past the employer was the exploiter, and sometimes continues to be even today, there is now a new danger, namely that a noble idea, which includes improvement in the position of the workers, has been diverted from its objective by those who seek the overturn of society” (Liakos 1993: 168).
It should nevertheless be noted that although the abovementioned rationale of Venizelos was laying the ground for long-term reproduction of capital, the representatives of the local bourgeoisie, at a loss to comprehend how times had changed, were evidently adopting a much more conservative stance. From this perspective, the position of the Greek delegation at the International Labour Conference in Washington in 1919 is characteristic: “In Greece the labour problem is affected by climatic conditions. The abundance of light, the clear skies, the dry atmosphere, the extreme brightness of the sun, inevitably make the worker there something different from the worker in a country further north. He cannot work with the same intensity and persistence, but on the other hand he does not feel comparable fatigue when working for more than eight hours. The effect of the good climate is also evident in the frugality of his lifestyle, which has always been characteristic of the Greek race. The quantity of food consumed by a Greek worker would seem insufficient to an American or European worker” (cited in Leontaritis 1980: 58-59).
Also of interest is the stance of the newly emergent workers’ movement towards these reforms. Its criticism focused on the inconsistency between the promulgation of laws and their routine violation. The view taken was that the bourgeois state could not withstand implementation of this legislation, which was why application of its most important components (for example the eight-hour work day) was deferred indefinitely (Fountanopoulos 2000: 333).
In the realm of health this period marks a significant turning point, namely the establishment for the first time of a separate Ministry of Health. As early as the time of his government in Thessaloniki, Venizelos had inaugurated the “Supreme Health Care Directorate” with responsibility for the health and welfare of the refugees, the disabled and other victims of the protracted warfare in which the country had been engaged. After prevailing over his opposition in 1917, assisted by the threat of cannon fire from French warships riding at anchor off Piraeus, Venizelos formed a government in Athens, subsequently proceeding to delink this Directorate from the Finance Ministry. It is characteristic of the confusion of these times that first the portfolio was determined and then afterwards the Decree “On the Competences of the Ministry of Health Care and the Organization of Health Services” (10/07/1917) was promulgated. In the corresponding debates in the Hellenic Parliament every type of contrary viewpoint was heard from parliamentarians expressing their skepticism of the new institutional framework that threatened to undo the process of “natural selection” that upholds the vigor of the nation! Notions of this type seem also to have had resonance in the stance of political personages when it came to the question of settling the refugees now arriving in Old Greece, something that could explain the similar reactions to the Decree of 10/07/1917 “On the care of refugees”, which entered into force at the same time as the Decree for establishment of the Ministry of Health Care. In 1918 the Section Head of the Finance Ministry K. Papakonstantinou, in a booklet printed at the National Printery, attempted to refute these views of individuals opposing state welfare on the grounds that it interferes with the “felicitous results of natural selection, whose tendency is to disencumber us of the weak, the infirm, the incompetent” (the quotation is from Kapanidis 1988: 92). Τhe same leitmotif was to be reiterated some time later after the Asia Minor Disaster on the subject, much larger in scale, of the refugees of the period 1922-1926. In this case infertile and disease-ridden sites for resettlement were selected systematically on the basis of precisely this criterion of step-by-step “natural selection” of those with the greatest “endurance”!
Implementation of health and welfare policies was thus anything but the considered demand of the Greek community of the day or indicative of the general social climate. This was even truer of the politicians that were its spokespersons. The climate was often one of confusion, lack of clarity in goals and orientations, and in some of its manifestations also of social callousness and transparent ignorance (for example knowledge of the non-hereditary character of tuberculosis dates back much further than the abovementioned extract from the parliamentary record). It was doubtless the dramatic and urgent external conditions (years of war and refugee movements) that necessitated the passing of some elementary measures, more so than the existence of a coherent hegemonic policy that the Venizelist governing centre was undertaking to carry out. This is in any case made abundantly clear by the expansion in the hospital care sector at this time: again it is Special Hospitals that obviously predominate, highlighting the isolationist proclivities of the public health policies under implementation. It was during this period that the hospitals for Sexually-Transmitted Diseases were established in Thessaloniki and Mytilene (1917), the sanatoria in Asvestohori, Syros and in Chania (1920), the Infectious Diseases Hospital in Mytilene (1918), with at the same time only a handful of general hospitals being opened for the purpose, primarily, of caring for the refugees, such as the one in Nea Ionia (1917), the “Evangelismos” of Kavalla (1919) and others, of charitable character, such as the “French” hospital in Lavrio (1919). The situation was to undergo dramatic change in the immediately following years, with a much larger wave of refugees flooding into Greece. Faced with the dimensions of the problems the Greek state would be forced within a very brief period of time to establish state hospitals in more than 35 towns throughout the country, with a capacity of over 2,638 beds, a very significant number when one takes into account that, on the basis of 1925 statistics, the total number of hospital beds in Greece did not exceed 9,000 (Kapanidis 1988: 126-127).
Whatever timid legislative measures were implemented to modernize the institutional framework for health care and welfare, they still fell far short of producing any result that could be detected statistically. The flu epidemic of 1918-1919, for example, spread death far and wide, particularly among the refugee populations. Infant mortality (which is considered among the most sensitive indicators of proper functioning of the health services) was probably aggravated rather than alleviated by the operation of institutions such as the Municipal Infant Asylum (“vrefokomeio”) of Athens (also known, not unjustifiably, as the “vrefoktoneio” [“infant butchery!”]), where between 1915 and 1919 3,920 deaths were recorded, i.e. 82% of those admitted. In the years that followed (1920-1924), with the much stronger social pressures that had come to prevail, the mortality rate in the said institution rose to 92% of its inmates, with other infant asylums in Greece recording mortality rates ranging from 50% to 99% (!) of the infants admitted to them. A similar picture emerges from the detailed report of the American Red Cross on Greek health care institutions in 1919 where attention is drawn to grave deficiencies in infrastructure, staff and medicines as well as to the inadequacy and unsuitability of supplies of basic foodstuffs (Kapanidis 1988: 56-57 and 252-262). Moreover, even the statute establishing the Ministry of Health focused primarily on the regulatory and supervisory functions of the state in existing hospitals, necessarily leaving out of account integration of the organizational and operational characteristics of hospitals for refugees, whether pre-existing or newly established. What was being repeated, in a way, was the scenario of Law 346/1914, as the meager financial resources of the Greek state, the many and varied counter-reactions, the political instability, the lack of provision for funding, the overly ambitious plans, all tended to frustrate implementation of much of what had been projected on paper. The application of a number of haphazard emergency measures to deal with the first wave of refugees from the Balkans Wars, without being integrated into the programming of the newly constituted Ministry of Health, led to a situation of chaos long before the Asia Minor Disaster. This state of affairs gave rise to the idea of a merger of the separate functioning services and agencies under the aegis of a single ministry. But though originating with the liberals, the idea proved impossible to get through the parliament until later, following Venizelos’ fall from power, when it was passed by the government of Protopapadakis-Gounaris-Stratos in the form of Law 2882 of 13/12/1922 “On reform and extension of the Ministry of Health under the new title of Ministry of Health and Social Welfare”.
To venture an overall assessment of the 1910-1916 period and the years between 1917 and 1920, there is arguably confirmation that whatever reforms took place in the health and welfare sector, they cannot be understood either as forms of bourgeois modernization or as product of the voluntarism of the Venizelos administration for the implementation of worker-friendly policies. The most notable feature of the first period is in reality the emergence of a demand for establishment of a minimum framework of social protection and the simultaneous attempt to keep that framework from going beyond certain limits, which is why so many exemptions were included, with the law on children and minors remaining essentially unenforced. Nevertheless, the continuing evolution of the workers’ movement, the establishment of the General Confederation of Greek Workers, the creation of the Socialist Workers’ Party of Greece and the resonance of the Bolshevik Revolution in Greek society were to generate still greater anxiety in the ruling classes and for this reason an attempt would be made to achieve further cutbacks in workers’ rights. Moreover, in the realm of health, the policies were to be fragmentary and governed by expediency, undermined by shifting goals, ideas and orientations, or by the uncertainty of funding for their implementation. The axis around which they appear to move was the supervisory and regulatory function of the state in a sector primarily humanitarian in character and the police-like repressive character of the interventions that were carried out. The first attempts at establishing a social state in Greece thus have much more to do with the state of the social forces at that specific social conjuncture than they do with the personal aspiration of one individual or a hazily modernizing orientation of the political centre.
5. The period between 1928 and 1932 and the creation of the Social Insurance Institute (ΙΚΑ.)[2]
The creation of ΙΚΑ, but also more generally the policy measures for health and welfare at that time, should be seen in correlation with the consequences of the global economic crisis and the effects it had on the Greek economy and society (Liakos 1988: 169-170), the additional labour power made available by the mass influx of refugees, and the restrictions on migration to the U.S.A. (and by extension shrinkage of migrant remittances) that resulted from the change in American migration policy from 1921 onwards (Vergopoulos [undated], p.341). At the same time the cost of living doubled and tripled (between 1922 and 1935 prices rose 207% and wages only by 83%), the daily wage contracted (between 1928 and 1932 it fell by more than 11%) and workers had great difficulty meeting their obligations. It is estimated that not even one quarter of working class families in 1930 were earning the minimum salary required to support themselves (Vergopoulos [undated] p.342). Unemployment skyrocketed from 75,000 unemployed in 1928 to 237,000 in 1932, i.e. around 40% of the wage-earning population (Sakellaropoulos 1991: 86-88). One significant parameter is the dynamic developed by the constantly spreading worker mobilizations that mark the period 1927-1931 (Livieratos 1987). We could mention characteristically that in 1927 the tobacco workers’ strike that led to clashes with workers being killed, injured and imprisoned, spread to other sectors, with the result that the Kafantaris government banned public meetings and created a wartime atmosphere with patrols in the streets and military guards at the premises of public utilities (Liakos 1993: 441).
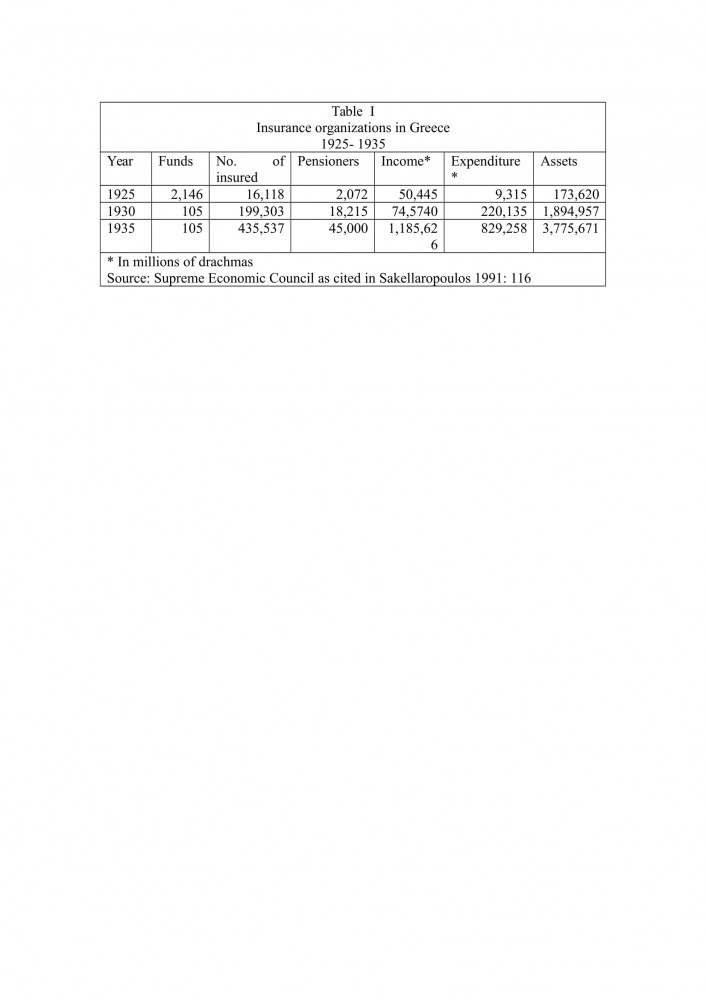
It should be clear from the above that the time had come for adoption of a series of social policy measures, quite apart from the fact that owing to the situation as a whole and to the need for social insurance structures, the number of insurance companies and insurance clients had risen dramatically, as is evident from Table I.
This dynamic led to the establishment of the Social Insurance Institute (IKA) by Venizelos in 1932 (Law 5733/1932). The objective was to organize a single insurance body for all wage earners that would give them protection from old age, sickness and infirmities – without this entailing provision against the problem of unemployment. In the Board of Directors of ΙΚΑ, there was provision for equal participation by representatives of both employers and workers, as well as three state officials, and an inspectorate to supervise the progress of the Institute. Finally, provision was made for future constitution of a Social Insurance Council to monitor the progress of social insurance and give its recommendations on the relevant ordinances to be promulgated. On the subject of funding the position was taken that the state would not be able to contribute to the social insurance budget and that the ideal was for social policy to be self-financing through subscriptions from employers and workers respectively in a ratio of 6.3% and 5% of the salary respectively (Tsalikis 2001: 37). There was accordingly a provision for existing capital to be channeled into the health programmes, into workers’ housing and into completion of production projects. This made it quite clear that the state was prepared to use the organization’s capital to fund the budget (Liakos 1993: 489-490).
Preparation for this particular law was programmed to take five months. Finally the coming to power of Tsaldaris in 1933 led to suspension of operations on the project and in the second year to the voting of Law 6298/1934 to reduce the level of contributions. The organizational procedures that had been programmed were completed after continual delays in 1937 and in December of the same year the Institute opened its doors in Athens, Patras and Thessaloniki. It was not until 1951, however, that it succeeded in covering the rest of the country (Tsalikis 2001: 44).
The conclusion to be drawn is that in the case of IKA the situation cannot convincingly be represented as a consequence of Venizelist radicalism or of some ill-defined bourgeois modernization. The objections raised by many different sectors in the power bloc (Tsalikis 2001: 38-40) not only contributed to delaying implementation of the law but also led to large numbers of important amendments being made. The ruling class evidently had very many serious misgivings about the way IKA had been brought into existence[3]. At the same time, the removal of operating costs from the state budget suggests that the state was seeking more to play the role of mediator between the two poles of society than to proceed with implementing broad income distribution policies. Last but not least, it is certain that if the preceding workers’ struggles had not taken place, the question of social insurance would have been posed in an altogether different manner.
To return to the field of health, the recomposition of a social entity with so many unresolved and urgent social problems had already been handled to some extent through direct state intervention. Thus, after 1925, the image of the country in relation to the interventions needing to be implemented in the health field had undergone radical transformation in the direction of reducing the involvement of charities and increasing the involvement of the state. In 1928 of the 9,936 available hospital beds, 5,285 were in state hospitals, 1,949 in municipal hospitals and 329 in university hospitals, with only 2,373 in hospitals run by charitable organizations. Fifteen years earlier the total number of hospital beds had been clearly smaller, and the proportions evidently skewed in favor of institutions of public benefit run by charities. This tendency was, as we saw above, the outcome of the events of 1923-1924, but is also observable throughout the entire period from 1924 to 1939. Proportionately, then, in 1922 the overall number of hospital beds had risen to an overall total of 11,742, in which 6,208 of them were concerning public health care institutions (Kapanidis 1988: 267-271).
The picture presented by the country in terms of indicators for health was nevertheless far from rosy. In his famous report “The problem of the death-rate in Greece”, published in 1940 in the Proceedings of the Academy of Athens, the “father” of Greek epidemiology V. Valaoras mentions that in the period between 1931 and 1935 Greece had the highest mortality rates of all the European countries from flu, typhoid fever, whooping cough, tuberculosis of other organs other than the respiratory system, and malaria. He also stated that Greece came a wretched second in mortality from scarlet fever, pneumonia and death in childbirth and fourth in mortality from tuberculosis of the respiratory system and gastro-enteritis. In absolute figures, mortality in Greece from a number of these diseases was twenty times higher than the corresponding figures for the developed European countries. And despite the fact that infant mortality was not mentioned as being extremely high by comparison with some other European countries, mortality among toddlers between one and four years of age and children from four to fourteen came to 32.7 and 4.7 per 1,000 respectively, putting Greece again in the first place in the relevant European comparative statistical listings. But even in the case of newborn babies, the distinguished epidemiologist questioned the validity of the state records, submitting more modest calculations, which nevertheless put Greece in the second or third position in the relevant European statistics, after Hungary and, perhaps, Bulgaria. The finding that Greece was last on the list for mortality from malignant neoplasms could likewise be given an unfavorable interpretation in the light of the well-known statistical correlation between cancer and communities of “abundance” and affluence (mentioned in Louros 1945: 21-33).
But at the institutional level, too, progress was slow, with much backtracking. Between 1920 and 1928 the Ministry of Health Care changed both ministers and orientation many times. It was abolished by the Pangalos dictatorship, only to be reconstituted later. The dengue fever pandemic of 1928, which afflicted Venizelos himself, was instrumental in heightening awareness of public health issues among politicians. On returning to government in 1928 Venizelos was to create the Sub-ministry of Health, which with the passage of Law 4172/1929 again acquired the status of a full ministry. During his brief time as Deputy Minister (1928-1929) A. Doxiadis was to appeal to the League of Nations, acknowledging on the one hand the enormity of the public health problem in Greece, on the other the inadequacy of national resources as a basis for dealing with it. The policy directives issued, at least in their manner of implementation by A. Pappas, now Health Minister, involved reductions in expenditure on hospitals and ancillary services and increases in expenditure on prevention, hygiene and the central supervisory services of the new ministry. This policy was only partially rescinded by Law 4737 of 07/05/1930 passed by the same government and bearing the eloquent title: “On financial support for public hospitals and similar legal persons of public law, etc”. With Venizelos’ fall from power in 1932 these contradictions in health policy were dramatically intensified[4] with the renewed abolition of the Health Ministry and some of its services in 1932 and recomposition of the again reunified Ministry of State Health Care and Welfare in 1933 (Kapanidis 1988: 99-101). One could therefore quite justifiably claim that these contradictions were key factors in the essential non-existence of stable policy-making right up until the outbreak of the mobilizations of workers and the general population in 1936, followed by imposition of the Metaxas dictatorship with its need to project social policy as a means of offsetting restrictions on political and social freedoms, and rights. Throughout the preceding period virtually all the country’s politicians seem to have been vacillating, swept up in the dramatic events of the day, with their even more dramatic effects on the health care needs of the population.
Thus, as with the preceding periods of the Venizelist government, so in the period between 1928 and 1932, whatever reforms took place were over-determined both by the particularities of the social struggles and by the very nature of the bourgeois state, which is able to enlist individual social demands to serve the objectives of long-term reproduction of capitalist relations.
6. Epilogue
In conclusion, and for the entirety of Venizelos’ term in office, it can be asserted that its raising came at a time in which previous provisos for welfare and health services in Greece were quite constraint. Moreover, definitely Venizelos’ administration apart from facing challenges of primary industrialization and modernization of Greek society had also to provide acute response to the outbreak of a huge humanitarian crisis inflicted by constant wars and their consequent massive immigration waves. On top, disputes on the directionality of policies to be introduced were constant in the both political and scientific circles creating, thus, discontinuities in robust policy implementation. In general, policy eventually pursued falls under the general rubric of bourgeois modernization but with much backtracking and contradiction that is sometime decisive for the final outcome in practice. Although the governing centre in many cases appeared to perceive the requirements of society and of the times, it was very far from embodying the strategy of a coherent and structured liberal ruling alliance: the contradictions appear to have permeated both the Venizelist camp and the opposing political groupings. Such fragmentation in political orientation might be explained on the grounds of contradictory character of directions (i.e. in strengthening or not social support or contrary natural selection) which were on debate at the time being. Such as abovementioned permeability of ideas, viewpoints and policies on public health, welfare and social policy, over-determined by the great political and social events of the day (wars, social conflicts) led to the phenomenon, familiar in any case in Europe as a whole, of a variety of institutional measures being carried out by conservative governments, despite having been proposed initially (but never fully implemented) by the liberal side of politics. The gradual “nationalization” of the hospital sector, its amalgamation with health and welfare services and the establishment of the country’s insurance system may be seen as examples of this. To put it in other words, the fragmented and multiply oriented totality of ideas and initiatives put forward during Venizelos’ era in Greece gradually was put into shape under the pressure of prevailing conditions also as reflected in public pressure for social welfare reforms.
The whole movement of the liberal side of politics per se seems to follow a trajectory ranging from collaboration with political radical political elements of the time (the “sociologists” Panastasiou, Delmouzos et al.) to attempting to place restrictions on the rising popular movement and its various forms of political expression. Although in general terms the course between 1909 and 1932 seems to be in the direction of development, it can in no way be described as direct or linear. More specifically, health policies implemented throughout the period under examination along with novelty and progressiveness are to some extent characterized also by repressive and restrictive conceptions expressed in individual measures taken either by the liberals or by other political centers. Despite that – and on the terrain where Venizelism shares a common course with sections of social and political radicalism – it was at this time that the concept of state responsibility for public health, for medical care and for welfare, was introduced onto the Greek political scene. The concept was to acquire even greater significance under the subsequent dictatorship of Metaxas. Additionally, throughout the period under examination, the social policy of the Venizelist government is typically characterized by a lack of correspondence between what exists on the statute books and what is applied in practice. The reasons for this lack of correspondence, apart from the internal conflicts within the liberals, are to be sought in the political instability of the time and in the consequences of the economic slump for Greek public finances. Constant changes in government as well as direction of implemented policies were reflecting a wider social and decision-making indecisiveness of the Hellenic society and its governance at the time being. As a result, many of the audacious reforms introduced by the Venizelists were to remain suspended in limbo or in a hybrid stage of implementation until the sharpening of social conflicts with the revolution of 1936 and the imposition of the Metaxas dictatorship effectively reordered the terms of the social contract in Greece.
In the final analysis individual people as such have a less determining influence on developments in the historical evolution of societies. What they tend more to do is to discern underlying trends, grasp situations before it is too late, lend concrete form to – and then promote - tendencies already existing in society itself and in the active contradictions and conflicting forces that comprise it. Certainly, Eleftherios Venizelos was an outstanding personage of bourgeois political life who was able to effect a distillation of the whole undertaking of national expansion and bourgeois modernization of the newly-created Modern Greek state. Indisputably, one part of this strategy was reconstitution of the social state and renewed concern for questions of health and welfare, much more so given the nature of the problems engendered by protracted wars and recurrent floods of refugees. But for the Venizelist camp the tendency shaping this policy was neither regular, nor socially homogenous, nor uniform: there were breaks and inconsistencies, leaps forward and backtracking, innovations and vacillations. At the same time, in an era of warfare, territorial expansion and the redrawing of borders, but also of frequent insurrections and revolutions within the geopolitical space of Europe, autonomy at the political level is similarly evident in the Greek social formation. Thus, with political instability an ever-present element, but also given the extent of the non-economic constraints that were the concomitant of such a period, the Venizelist centre was able to realign relations at the political and economic levels, in this way reinforcing the historic role retrospectively attributed to it. Further historical and social research may shed light on the specific terms and conditions of implementation of the critical political choices made at that time, and on the individual decision- making centers that contributed, in whatever way. In any case, schematic representations of Venizelism either as a generalized social radicalism or as an entirely bourgeois mode of government should perhaps be abandoned in favor of a more nuanced approach. Moreover, the deeper reasons for politicians elaborating policies for health, welfare and social policy at that time must be sought more in the social processes, the conflicts and the realignments of the time and less in individual interventions, which may have broadened the horizons of the political agenda but in no way influenced it decisively.
BIBLIOGRAPHY
Α. GREEK
Flountzis A., 1983, Τhe student movement: 1923-1928, Athens: Kedros.
Fountanopoulos K., 1999, “Wage Labour” in Christos Hadzijosif (editor), History of Greece in the 20th Century. The beginnings 1900- 1922, Vol. I, Athens: Bibliorama, pp. 87- 121.
Fountanopoulos K. 2002, “Labour and the Workers’ Movement in Greece” in Christos Hadzijosif (editor): History of Greece in the 20th Century. The Interwar Period 1922-1940, Αthens: Bibliorama, pp. 295 – 335.
Hadjijosif C., 1988, “The Venizelist Opposition to Venizelos and Political Reconstitution (-ism) in the Interwar Period” in G. Mavrogordatos and C. Hadjijosif (eds.) Venizelism…. pp. 439-458.
Hering G., 2004, The Political Parties in Greece 1821- 1936, Volume II, Athens, National Bank of Greece Cultural Foundation.
Kalliga E., 1990, Child Welfare in 19th Century Greece, Αthens-Ioannina: Child Research Foundation/Dodoni.
Kapanidis N., 1988, Closed Treatment in the Modern Greek state (1909-1940), Doctoral thesis, Thessaloniki.
Kordatos G., 1972, History of the Greek Workers’ Movement, Athens: Boukoumanis.
Koukoules G., 1984, Greek Trade Unions: financial self-sufficiency and dependence, 1938-1984, Athens: Οdysseas.
Leontaritis G., 1980, “The Greek workers’ movement and the bourgeois state 1910-1920” in T. Veremis and O. Dimitrakopoulos (eds.), Studies on Venizelos and his Era, Athens: Filippotis, pp.49-84.
Levett J., 2008, “The foundation of Athens School of Hygiene”, in Kyriopoulos J., (ed.), Public Health and Social Policy: Eleftherios Venizelos and its era, Athens, Papazisis, pp. 113-120.
Liakos Α., 1988, “From the guardian state to the welfare state: The parameters of workers’ politics in the Inter-War period”, in Symposium on Eleftherios Venizelos, Athens: Hellenic Literary Society and Historical Archive – Benaki Museum, pp. 169-185.
Liakos Α., 1993, Labour and Politics in Greece in the Interwar Period. The International Office and the rise of social institutions, Athens; Research and Education Foundation of the Commercial Bank of Greece.
Livieratos D., 1987, Social Struggles in Greece (1927-1931). Out of contempt a new dawn, Αthens; Kommouna.
Lixouriotis G., 1988, “Protective legislative interventionism and the emergence of labour law in Greece: The case of child labour” in G. Mavrogordatos and H. Hatzijosif (eds.), Venizelism…, pp. 205-223.
Louros Ν. Κ., 1945, National Health Care Organization: A Plan, Athens: Papagiannidis.
Mavrogonatou G., 2008, “Cultural assertion of water supply network in Athens during the period 1880-1930. The dimension of hygiene in public and private sphere”, in Kyriopoulos J., (ed.), Public Health…, pp. 197-214.
Mavrogordatos G., 1988, “Venizelism and Bourgeois Modernization” in G. Mavrogordatos and H. Hatzijosif (eds.) Venizelism…, pp. 9-19
Mavrogordatos G. and H. Hatzijosif (eds.) Venizelism and Bourgeois Modernization, Heraklion, University editions of Crete.
Moudopoulos S., 1988, “Law 281/1914 on professional associations and its effects on the development of the trade-union movement” in G. Mavrogordatos and H. Hatijosif (eds). Venizelism…pp. 225-253.
Pefanis P., 2004, Comprehensive History of Medicine, Athens, Exantas.
Sakellaropoulos T., 1991, Economy, Society, State in Interwar Greece, Athens: Pliroforisi (Information)
Skoutelis G.D., 1990, Social Insurance: Development and Crisis, Athens: Centre for Social Science of Health.
Troumbeta S., 2008, “Eugenics’ responses to modernization challenge of Hellenic society (1900-1940)”, in Kyriopoulos J., (ed.), Public Health…, pp. 335-355.
Tsalikis G., 2001, “The foundations of (anti)-social insurance in Greece (1840-1940)” in G. Kyriopoulos et al (eds.) Health insurance in Greece, Αthens: Themelio, pp. 19-47.
Τsalikis G., 2008, “The first and second law on IKA: the position of the Liberals and the Populists on social insurance in the interwar period” in the collective volume Public Health and Social Policy: Eleftherios Venizelos and his age, Αthens, Papazisis, pp. 421-434.
Tsiros N., 1997, Τhe legislative work of Eleftherios Venizelos in the 1911-1920 period in the context of his reform policies and the socio-political realities of the time, Αthens: Αnt. N. Sakkoulas Editions.
Τzokas S., 2002, Eleftherios Venizelos and the project of bourgeois modernization 1928-1929. Building the Bourgeois State, Athens: Themelio
Vergopoulos, K., (no date), “The Greek Economy from 1926 to 1935”, in History of the Greek Nation, .vol. 15, pp. 327-342
Weindling P., 2008, “The League of Nations, the Rockefeller Foundation and Public Health in Europe in the Interwar Period”, in Kyriopoulos J., (ed.), Public Health…, pp. 79-96.
Zilidis C., 2008, “Epidemiological reality in Greece in the interwar era and policy for re-organization of health services”, in Kyriopoulos J., (ed.), Public Health…, pp. 131-149.
Β. FOREIGN LANGUAGE
Abel-Smith B., 1964, The Hospitals: 1800-1948, London: Heinemann.
Ackerknecht E. H., 1998, History of Medicine, Greek translation: Paschalis-Iliadis, Athens: Marathia.
Baer H. A., 1989, “The American dominative medical system as a reflection of social relations in the larger society”, Social Sciences & Medicine, 28 (11), 1103-12.
Bale A., 1989, “Medicine in the industrial battle: early workers’ compensation”, Social Sciences & Medicine, 28 (11), 1113-20.
Baymun W. F., 1988, “Ideology and Health Care in Britain: Chadwick to Beveridge”, Publ. Stn. Zool. Napoli II, 10 suppl., 75-87.
Ehrenreich D., English D., 1979, For their own good: 150 years of the experts’ advice to women, New York: Anchor Press/Doubleday, Garden City.
Elling R. H., 1994, “Theory and method for the cross-national study of health systems”, International Journal of Health Services, 24 (2), 285-309.
Fox D. M., 1986, “The consequences of consensus: American health policy in the twentieth century”, Milbank Quarterly, 64 (1), 76-99.
Gough I., 1979, The Political Economy of The Welfare State, London: Macmillan.
Gramsci A., 1949, Gli Intellettuali e l’ organizzazione della cultura (“Oi Dia nooumenoi”, Greek translation: T. Papadopoulos, Athens: Stochastis, 1972.
Honigsbaum F., 1990, “The evolution of the N.H.S.”, British Medical Journal, 301 (6754), 694-9, Oct. 3.
Knowles J. H., 1973, “The Hospital”, Scientific American, 229 (3), 128-138, Sep.
Navarro V., 1975, Medicine under Capitalism, New York: Prodist.
Rodberg L., Stevenson G., 1977, “The medical care industry in core capitalism”, The Review of Radical Political Economics, vol.9 (1), Sping.
Silver G. A., 1987, “Virchow, the heroic model in medicine: Health policy by accolade”, American Journal of Public Health, 77, 82-88.
Waitzkin H., Waterman B., 1974, The exploitation of illness in capitalist society, Indianapolis: Bobbs-Merril Co.
White W. D., 1990, “The “corporation” of U.S. hospitals: what can we learn from the nineteenth century industrial experience?”, International Journal of Health Services, 20 (1), 85-113.
[1] The Decree was followed by institutional measures for insurance against sickness in 1833, for work accidents in 1884, for old age and infirmity in 1899, death in 1911 and unemployment in 1927. Similar regulations were also established for other countries, such as the introduction of insurance against sickness, infirmity and unemployment in England in 1911 and in France with equivalent legislation in 1928 and 1930 (Skoutelis 1990: 27,42)
[2] Above and beyond the creation of ΙΚΑ, during that four-year period in office, the Venizelos government proceeded to establish the Ergatiki Estia (1931), which aimed at establishing accommodation for workers. But the construction of living quarters was secondary and supplementary to the basic goal of controlling trade unions through controlling housing (Koukoules 1984: 51)
[3]Venizelos himself waged a great struggle to persuade people that this approach contributed to protecting the bourgeois order, and to reassure the recalcitrant industrialists: “To return, however, to the promise I made that I will persuade the industrialists reacting against these changes that it is in their interest to support them, I say this: if the introduction of social insurance necessitates a 4% additional outlay on workers’ wages, they should realize that if they manage to escape just one major strike demanding higher wages, they will have more than covered the expense entailed for them by the further 4% they would be paying for the securing of social insurance. It is obvious that institutionalizing social insurance is a way of ensuring fewer strikes in the future than we will have if we do not introduce this reform.” And elsewhere: “My words are primarily addressed to the world of employers, because – as I think I am entitled to say – if I have been widely calumniated for being of the Left and excessively pro-working class, I nevertheless belong to the bourgeoisie and it is not possible to impugn my good faith when I declare that I serve, by whatever means appropriate, the existing social order (cited in Tzokas: 191-193).
The criticism emanating from employers’ circles was that through his promises to the working class Venizelos was contributing to the exacerbation of class struggle, making him in effect responsible for labour unrest. The view of the business world was that the repressive mechanisms of the state were adequate for holding the working class in check so that there was no need for handouts and promises (Tzokas 2002: 193). At a meeting of the Chamber of Commerce and Industry (16th-19th February 1930) a recommendation was made to the government that no new insurance funds should be created and existing ones should be abolished (Tsalikis 2008: 428). At the Fourth Congress of Chambers of Commerce and Industry in 1931 the decision was taken to declare that the business world would accept the expediency of social insurance, but only for workplace accidents, while at the same time rejecting insurance against sickness and demanding that insurance against old age and disability be subject to rigorous scrutiny (Liakos 1993: 494).
Reactions were to be seen also at the level of politics qua politics, for the law was passed only by the Venizelists. The opposition abstained en bloc, challenging its financial underpinnings. It took the view that the burden to the Greek economy would be much greater than what was projected in the preamble to the legislation. What was proposed instead, without questioning of the importance of social insurance, was another system where the emphasis would be more on IKA, the Social Insurance Institute, which would be required to incorporate a greater number of individual funds, with less involvement from the state (Liakos 1993: 502).
[4] It is important also to examine the reactions of workers to these reforms. They can be divided into two categories. The first includes those already insured in industry or company funds. The second concerns organizations on the left side of political spectrum and relevant to workers’ collective interests (chiefly the General Confederation of Greek Workers [GSEE] and the Greek Communist Party [KKE]).
More specifically, workers enrolled in industry funds did not wish to be covered by IKA. They judged that notwithstanding the higher cost of insurance they were able to exercise control over the management of their reserves. In addition to this, unlike IKA, a number of funds - such as those of the bakers or tobacco workers - provided for insurance against unemployment (Liakos 1993: 496).
The General Confederation of Greek Workers, which had undergone contraction owing to the defection of the forces adhering to Greek Communist Party politics, demanded that reforms be accelerated. They resisted the prospect of amendments under the pressure of lobbying from private insurance companies and other business interests (Liakos 1993: 497).
The strongest reactions came from the milieu of the KKE. According to the Unifying General Confederation of Workers, the confederation established by Communist workers “Nothing leads to the conclusion that Venizelos wants to institute social insurance fund. On the contrary, all this shows that Venizelos has no intention of establishing social insurance funds because the capitalist oligarchy, of which he is a representative, has nothing to gain from them being established. Particularly today with the crisis it is not inclined to “waste” money in this way because even in other countries where social insurance systems have been in operation for years the capitalist establishment there is constantly downgrading them and even abolishing them. The simple fact is that the Venizelos government is deceiving the workers” (Liakos 1993: 499). Apart from this, on more specialized questions too they condemned the government for not including unemployment insurance, for imposing through workers’ contributions a form of taxation on the working class, for allowing sickness and disability benefits and pensions to remain at very low levels, for restricting insurance just to certain categories of worker (those in stable employment and living in the large urban centres) (Liakos 1993: 499-500).